Medical Education for Visual Learners
Hypothermia ECG Explained
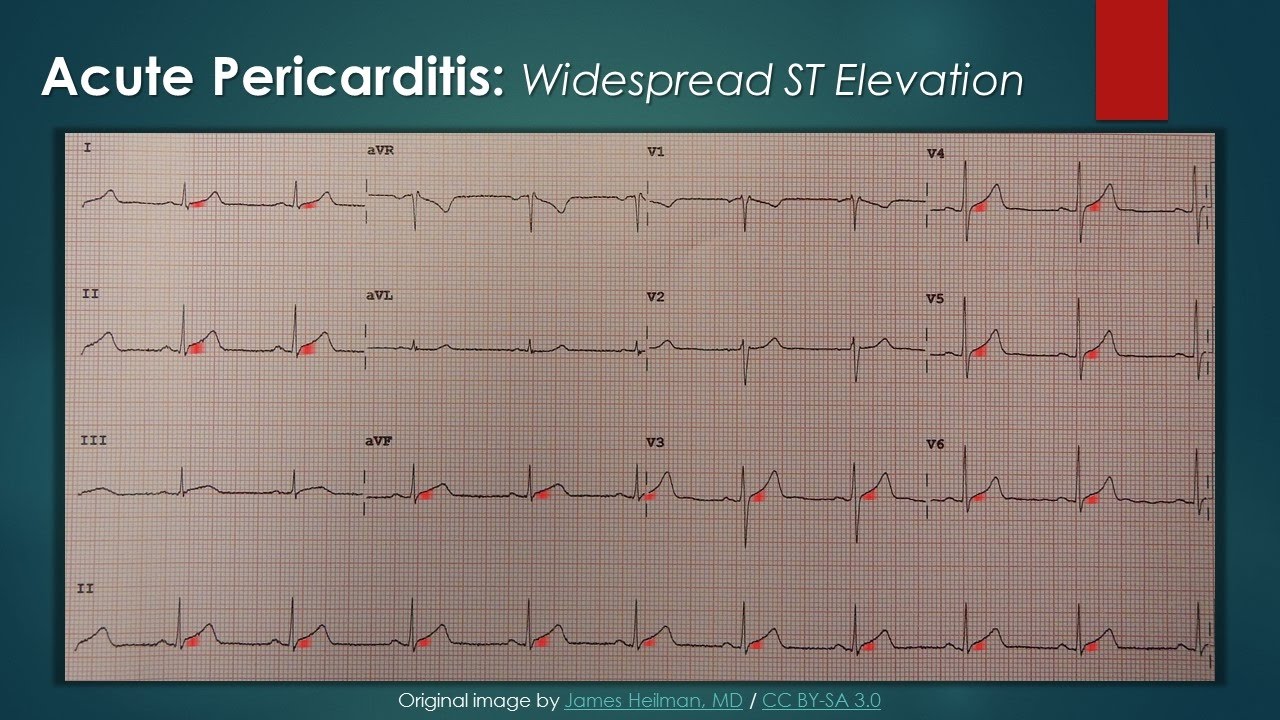
A classic ECG finding in hypothermia is J Point Elevation (a.k.a., Osborn J wave). Note the prominent convex deflection at the junction of the QRS complex and ST segment. It is most clearly evident in the precordial leads and typically negative in leads aVR and V1. The amplitude of the J wave roughly correlates with the severity of hypothermia. Although J waves are characteristic of hypothermia, they can also be present in Brugada syndrome, benign early repolarization, hypercalcemia, sepsis, and subarachnoid hemorrhage.
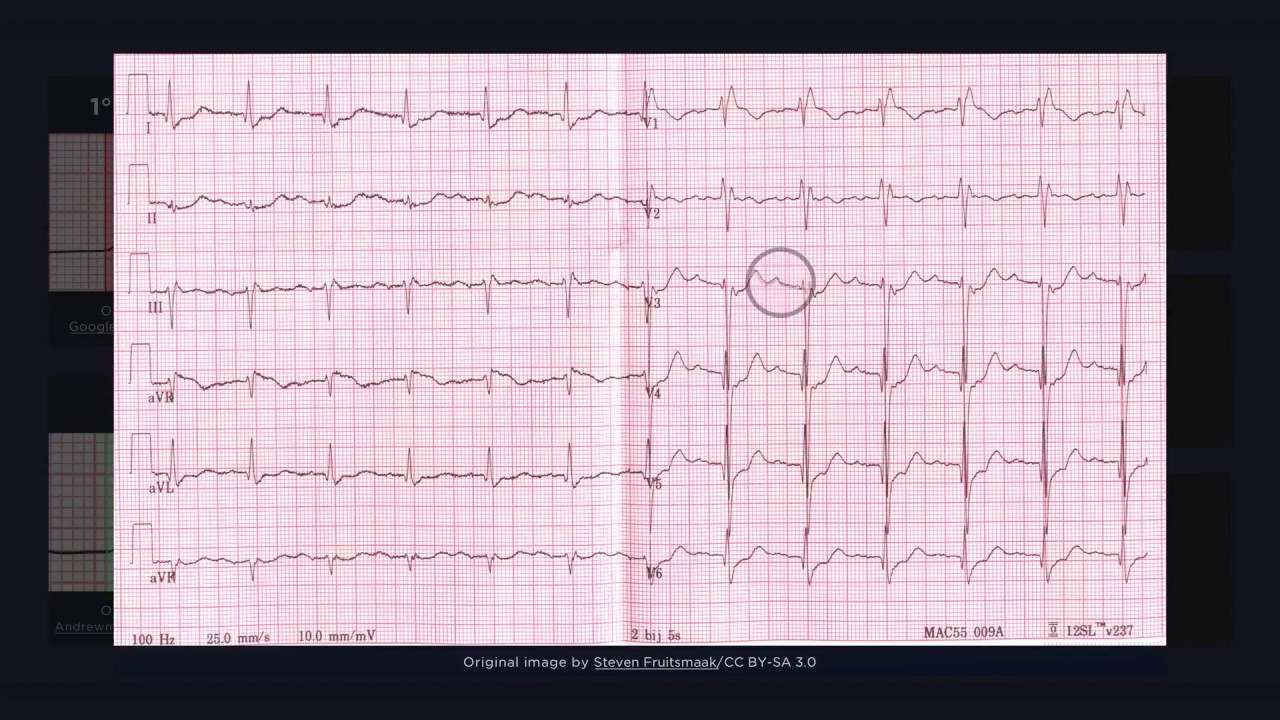
Hypothermia can also cause diffuse slowing of impulse conduction. This can lead to prolonged intervals (e.g., PR, QT) and widened waveforms (e.g., p waves, QRS complexes). Inspect the QT interval in this ECG. The PR interval and P waves cannot be assessed due to the underlying rhythm.
As well, marked slowing of the heart rate can occur due to a variety of bradyarrhythmias (e.g., sinus bradycardia, AV block, atrial fibrillation with slow ventricular response). In this ECG, Note the irregular R-R intervals and fibrillatory waves of A-Fib, yet the slow ventricular rate. One pitfall to be aware of, however, is that shivering can lead to electrocardiographic artefacts (e.g., waves simulating ventricular tachycardia).
0:00 J-point Elevation "Osborn J wave"
0:42 Slowed Conduction
1:08 Bradyarrhythmia
1:30 Pitfalls
📺 Subscribe To My Channel and Get More Great Quizzes and Tutorials
https://www.youtube.com/channel/UC95TzSH1B_2EjaZMgDBNmvA?sub_confirmation=1
#FOAMed #cardiology #ECG
Disclaimer: All the information provided by Medical Education for Visual Learners and associated videos are strictly for informational purposes only. It is not intended as a substitute for medical advice from your health care provider or physician. It should not be used to overrule the advice of a qualified healthcare provider, nor to provide advice for emergency medical treatment. If you think that you or someone that you know may be suffering from a medical condition, then please consult your physician or seek immediate medical attention.